How Accessible is Health Care in Your County?
June 18, 2007
PAER-2007-3
Eda Unal, Graduate Student; Susan Chen, Assistant Professor and Brigitte Waldorf, Professor
![]()
![]()
![]()
![]()
![]()
High quality and easily accessible healthcare services are essential for the well-being of Indiana residents. Health care services also influence economic prosperity. Research has shown that availability of health care services does play a role when firms decide where to start a new business. Health care accessibility is a multi-faceted concept. It embraces such diverse issues as whether health care is affordable or covered by health insurance, whether it is available within a reasonable travel distance, and whether it is available at all times to all people. The research reported here focuses on the geo- graphic aspects of accessibility. Does where one lives make a difference in how easily health care facilities and physicians can be reached? In other words, does location matter when it comes to health care accessibility?
In 2005, a total of 13,283 physicians served Indiana’s 6.2 million residents. That is, one physician for every 469 Hoosiers. This is slightly worse than for the nation as a whole where one physician is shared by 442 Americans (see Figure 1). Focusing only on Indiana, some counties do much better than the national average. For example, Marion County has one physician for every 254 residents. This does not take into account that Marion County physicians may also serve patients living somewhere else. For example, patients who live close to Marion County may find it relatively easy to access the rich medical care that Marion County offers.
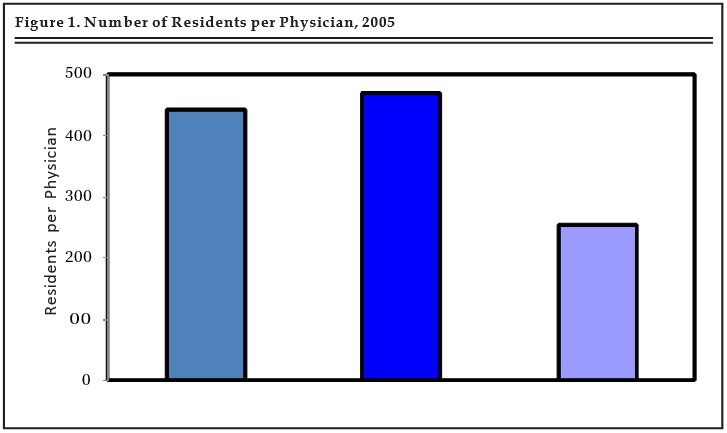
Figure 1. Number of Residents per Physician, 2005
To get a better idea of differences in access to medical care across the state, we calculated how accessible medical care is in each county. The calculations consider the health care services in the county of residence, medical services offered in other Indiana counties, and the distances that residents must travel to reach medical services. In our method of determining how accessible health- care in a county is the county with the best access to medical care receives a score of one. The county with the worst access to medical care receives a score of zero. Every other county gets a score between zero and one. The closer the score is to one, the better the county’s access to health care. We performed the calculations twice: once for access to physician care, the second time for access to hospital care.
Access to Physician Care
Access to physician care is very unequal across Indiana counties (see Figure 2, Table 1). The darkest shading indicates the best access and the lightest colors indicate poor access. Marion County has the most favorable access to physicians. Good access to physician care is also recorded for regional centers, such as Vanderburgh County (Evansville) and Allen County (Fort Wayne), the two counties housing Indiana’s major universities (Tippecanoe and Monroe counties), and the fast growing suburban counties of Indianapolis (Boone, Hamilton, Hancock, and Hendricks counties).
At the other end of the spectrum, Posey County in Southern Indiana has the worst access to physicians. It is closely followed by four other rural counties located along the Ohio River, namely Switzerland, Ohio, Perry, and Spencer counties. Only two of the ten counties with the worst physician accessibility, Benton and Newton counties, are located in the northern portion of the state. They are part of a vast rural area along the Illinois border that has also been identified as a Health Professional Shortage Area by the Department of Health and Human Services.
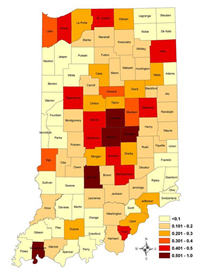
Figure 2. Access to Physician Care in Indiana Counties
Access to Hospital Care
Five counties that make the top-ten list of best access to physician care also show up on the top-ten list of best access to hospital care: Marion, Vanderburgh, Monroe, St. Joseph, and Allen counties (see Figure 3 and Table 2). New to the top-ten list are some urban counties that serve as regional centers for the surrounding rural areas: Vigo County (Terre Haute), Jefferson County (New Albany), Lake County (Gary), Madison County (Anderson), and Porter County (Portage, Valparaiso). Note that five counties that provide an abundance of physician care do not show up on the top-ten list of best access to hospital care: namely Tippecanoe County and the four suburban counties of Indianapolis (Hamilton, Hancock, Hendricks, and Boone counties).
The most underserved counties with poor access to hospital care are listed on the right-hand side of Table 2. The concentration of poor access to hospital care in the southern rural portion of Indiana – especially along the Ohio River – is extreme. Only one county on the list, Benton County, is located in Northern Indiana. Seven of the top-ten 10 counties with poor access to hospital care also appear on the top-ten list of worst access to physician care, and are thus double-disadvantaged: Benton, Crawford, Ohio, Perry, Posey, Spencer, and Switzerland counties.
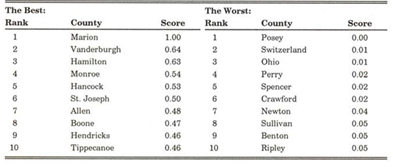
Table 1. Indiana Counties with Best and Worst Access to Physician Care
Who Lives in Counties with Poor Health Care Access?
Identifying the counties that have poor health care access is very important to ensure that resources are directed where they are needed. It is equally important to identify vulnerable population groups who live in areas with insufficient health care access. Comparing the population in the counties with best health care access to the population in the counties with worst access, our study shows that:
- The elderly are slightly over-represented in areas with poor access to health care.
- Children under five are slightly over-represented in areas with good access to health care.
- The population in areas with poor access to health care is almost exclusively white. In contrast, the population in areas with good health care access is much more diverse, with about 20% of the population being non-white.*
- Farm employment in the area with poor health care access makes up almost 8% of total employment, but is nearly absent from areas with good health care access.
- The average per capita income is substantially lower in the area with poor health care access than in the area with good health care access. The difference amounts to more than $5,000.
- Residents in the area with poor access to health care are, on average, less educated than the residents of the area with good health care access. The percentage of residents with a college degree is more than twice as high in good compared to poor health care accessibility areas. At the other end of the educational attainment scale, persons without a high school degree are strongly over-represented in the area with poor health care access.
* This does not imply that the non-white population has better access to medical care than the white population. For example, the U.S. Department of Health and Human Services has designated a portion of Marion County as a Health Professional Shortage Area. In that area, the population is predominantly non-white.
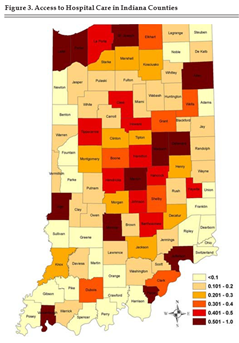
Figure 3. Access to Hospital Care in Indiana Counties
Concluding Remarks
Equal provision of healthcare services for all people in all parts of Indiana
is a challenge to policymakers. Our research shows that Indiana’s rural counties turn out to be the most poorly served places when it comes to health care. This is an inconvenience for everybody living in these areas. It is also a heavy burden for the elderly, those who are suffering
from chronic disease such as diabetes, and pregnant women needing pre-natal care. Insufficient access to health care can be fatal in cases where patients need immediate medical attention. For example, patients suffering a heart attack require medical care within an hour to increase survival chances and to avoid permanent damage to the heart. Insufficient access to care can also deter people from seeking preventive care resulting in more expensive treatments in the long run.
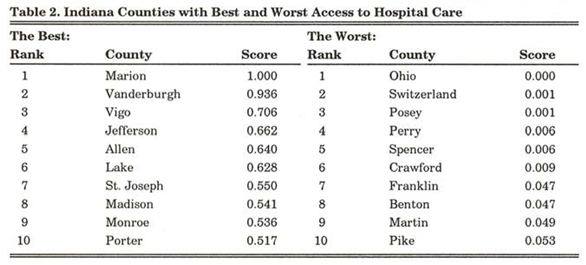
Table 2. Indiana Counties with Best and Worst Access to Hospital Care
Health care services in remote rural areas can certainly be improved by increasing the number of physicians in the affected counties, along with increasing the number of Rural Health Clinics and extending their services. But we also recommend strategies that make it easier for rural residents to access excellent health care services in urban areas in Indiana. Extending the ambulance service, including airlifting patients needing emergency care, is just one example. However, we may also look to new technologies allowing remote access to the expertise of physicians and hospitals in urban centers.
![]()
![]()
![]()
![]()
![]()
